Vaccine Hesitancy Isn't the Whole Story
When it comes to Black communities in New Haven and COVID-19 vaccination, the problem of vaccine inequity is larger than vaccine hesitancy.
On Feb. 5, I listened in as members of the Dixwell Avenue Congregational United Church of Christ bantered about the impending snowstorm. From the comfort of their homes, they asked about each other’s days, shared how their family members were doing and complained about laying salt and shoveling snow. I was a newcomer, but the group quickly embraced me, asking how I was doing and how I was related to the church. I was there, I said, to talk to them about their thoughts on the COVID-19 vaccine.
The 20 or so congregants had been gathering over Zoom as part of the church’s wellness series for months now. Senior Pastor Frederick Streets, a longtime New Haven resident, said the church leadership was inspired to organize the Zoom series once it became clear that traditional Sunday services could no longer fully engage the community. He sought a different way to increase social connectedness.
Beyond fellowship, the meetings became a place to share COVID-19 updates. The church invited public health experts, such as New Haven Health Department Director Maritza Bond and her staff, to the meetings, where they personally addressed questions about the virus — and more recently, the vaccine.
On the evening I attended the weekly Zoom, Connecticut’s vaccine rollout was already underway. Those who were vaccine-eligible described their ease in registering for vaccination. One member reported, “I called on a Friday afternoon, and I got an appointment for Monday.” Other congregants expressed doubt about the vaccine’s efficacy due to its swift development, a concern that prompted murmurs of agreement among the attendees.
(Frederick Streets)
According to a January 2021 report by the nonpartisan Kaiser Family Foundation, 43 percent of Black Americans said they would “wait and see” if offered the COVID-19 vaccine — the highest percentage of any racial group. The same study found that only 3 percent of Black Americans had received at least one dose of the vaccine, the lowest percentage of any racial group. Current Connecticut statistics report that, as of March 8, only 6.1 percent of non-Hispanic Black residents 16 years and older have been fully vaccinated compared to 14.1 percent of white residents in the same age group.
Lower vaccination rates within Black communities are often attributed to vaccine hesitancy. However, health equity experts point out that vaccine hesitancy isn’t the whole story. In New Haven, and nationwide, structural racism contributes not only to medical distrust but also to a lack of vaccine access and information within Black communities.
SYSTEMIC MEDICAL RACISM
Vaccine hesitancy can partially be explained by deep-rooted mistrust borne from repeated instances of medical racism, according to Jessica Cerdeña, an M.D. and Ph.D. student in medical anthropology at the Yale School of Medicine and researcher on race and racism in medicine.
“If you were to go and talk to a typical medical professor and say, ‘Do you think about patients differently because of their race?’ they would say, ‘No, that’s racist,’” Cerdeña said. “But if you go through their lecture slides, if you go through their case studies, you’ll see consistent patterns by which patients are thought about differently because of their race.”
Cerdeña raised the example of focal segmental glomerulosclerosis (FSGS), a kidney disease for which being Black or Hispanic is commonly thought to be a risk factor. When a Black or Hispanic patient comes in with excessive protein or blood in their urine, Cerdeña said, a doctor has been conditioned to assume that they have FSGS. As a result, doctors are more likely to falsely diagnose them with FSGS and overlook their true medical problem. The deeper problem is that the assumption is substantiated by the falsehood that race is a biological category instead of a “socio-political category” that was “developed to justify political prerogatives,” Cerdeña said.
These “political prerogatives” started centuries ago, Cerdeña explained. Doctors on ships that transported captured Africans conducted invasive medical exams and procedures that were intended to increase their economic value. In 1932, the U.S. Public Health Service began administering false syphilis treatment to 600 Black men, 399 of whom had the disease, in the “Tuskegee Study of Untreated Syphilis in the Negro Male.” For over 40 years, they studied the disease’s progression and even withheld penicillin after it became the known cure. This evidence of abuse at the hands of U.S. federal agencies is widely cited as an explanation for the African American community’s distrust of health care.
“We remember the past… but we don’t live [in the past]. It’s historical for us: It makes us vigilant, but it doesn’t make us stupid.”
—Rev. Leroy Perry
Cases of racist medical abuse persist in contemporary times. This past December, Indiana resident Dr. Susan Moore died after her case of COVID-19 was not taken seriously by white physicians within the Indiana hospital system. The story caught the attention of national media outlets only after Moore posted her personal testimony to social media.
New Haven is no different. According to Doris Dumas, president of the Greater New Haven NAACP, New Haven was vulnerable far before the COVID-19 pandemic. Almost 10 years ago, the Greater New Haven NAACP published its “Urban Apartheid Report,” which outlined what Dumas called “the two New Havens.”
Dumas said that New Haven COVID-19 death rates are currently 25 to 50 percent higher in Black and brown communities than in white communities. “We can pinpoint the red areas where there are the highest numbers,” said Dumas. “Certainly, we are advocating that our communities need to be a priority with as many people having access to getting the vaccine and having information about the vaccine.”
Tackling hard topics like the Tuskegee experiment is an integral part of discussions surrounding mistrust within the community, said Dumas. “We see a lot of [mistrust], and it’s justified,” Dumas said. However, Dumas was optimistic that mistrust can be curbed. “I think you combat it with having as many conversations, forums and discussions on the facts,” she said. “And also not just [dismissing] concerns, but [addressing] them and [letting] people know that there’s a long dark history with this and it’s real in our community.”
CONTEMPORARY HEALTH CARE PRACTICES
Dr. Keith Churchwell, president of Yale New Haven Hospital (YNHH), said the key to fostering community trust is taking a more aggressive stance on sustained care after inpatient treatment. According to Churchwell, YNHH has prioritized equity by emphasizing the patient’s “overall symptomatology” over “the subjective evaluation of a clinician or nurse.” As a result, during the COVID-19 pandemic, YNHH rates of morbidity and mortality for African American and Latino inpatients have actually matched or been less than the rest of the population, Churchwell said.
However, extending care into the patient’s everyday life is not the hospital’s expertise, he said. “How do we address not only the issues of [a Black patient’s] acute medical illness, but all the [social determinants of health] that we know have an impact on their medical issues?” Churchwell asked. “We, in the past, did not address that to the degree that it needs to be addressed.”
(Regina Sung)
Tackling this key question is also a concern for medical researchers at the Yale Center for Clinical Investigation (YCCI), a program for clinical research that aspires to improve patient care. The YCCI began their Cultural Ambassadors program in 2010 as an effort to increase the number of people of color participating in clinical trials. Tesheia Johnson, director and chief operating officer of YCCI, described the program as a “bi-directional partnership,” with the communities it supports being equal partners in the planning process.
Cultural ambassadors, who serve as “expert resources” for the program, hail from the AME Zion Church and Junta for Progressive Action, the oldest Latino community-based nonprofit in New Haven. “It’s been this great relationship that we’ve had over the years and they really have made a huge difference in the clinical research at Yale,” said Johnson. Before the pandemic, Johnson said, over 30 percent of total participation came from minority groups. When the Cultural Ambassadors were specifically engaged in a study’s design, that percentage ranged from 40 percent to 90 percent.
Onyema Ogbuagu, associate professor of medicine at the Yale School of Medicine, is a principal investigator on several COVID-19 clinical trials through YCCI and a close cultural ambassador collaborator. When it comes to vaccine development, “The question most people ask is, ‘Did they include people like me?’” he said. “That could mean either people like me, meaning my race or ethnicity, or people like me, meaning my comorbidity or medical history profile.” The Cultural Ambassadors program, then, aims to be a bridge between under-represented minority communities in New Haven and research programs whose positive impact on those communities hinges on their participation in studies — including recent vaccine trials.
AGE AS A FACTOR
Ogbuagu noted that when engaging people in clinical trials, a “huge currency” is “established trust and credibility.” Within minority communities, this trust appeared decidedly skewed towards older individuals. “In some way, I find that the older people tend to be a little more trusting of the system than younger individuals,” said Ogbuagu. “I’m not sure if it’s trust that’s derived from wisdom or past experience.”
He noted that this observation among minorities was from his Yale-affiliated point of view. “It’s hard because I think that the key people we interacted with were some of the cultural ambassadors,” said Ogbuagu. “So these guys have had a much more long-term relationship with the research program.”
“We don’t have the privilege of saying we can just wait this out because it’s affecting us in such a radical way, more so than our counterparts.”
—Rev. Leroy Perry
His observation was seconded by the Rev. Leroy Perry, pastor of St. Stephens AME Zion Church and a longtime cultural ambassador. Perry has observed varying levels of trust within different age groups of his constituents. “I think that elderly people in the African American community have shown that they are willing to take this vaccine, and it has nothing to do with a medical apartheid,” he said.
“You have younger kids who are in elementary school and grade school who are saying, ‘Grandma and grandpa, mommy, I want to take the shots so we can go back to going to school every day and having life as normal.’” He continued, “Then you have another group of people who are somewhere in between that, the late 20s to mid-50s population, who are saying, ‘I want to wait and see, I don’t really know, I don’t really trust them.’”
This “wait and see” approach among the young adult cohort makes sense to Ogbuagu, who noted that the “hesitance” we are observing in young people “may not necessarily be reflective of frank reluctance to take the vaccine.” Rather, the priority groups in vaccine rollout may be a “systemic way of telling young people you’re not a priority.”
Ogbuagu said that the priority groups aren’t misguided, but they certainly don’t encourage a hesitant young person to go out of their way to get the vaccine. “Because of the disproportionate impact [COVID-19] is having on older individuals, you can imagine that an individual’s personal risk assessment — ‘What’s my risk of getting COVID-19 and dying?’ — is a very different calculation for a young individual than an older individual,” said Ogbuagu. “And in some sense you could argue, if you perceive yourself to be a young person at the lower risk, it’s not the worst idea to want to delay the vaccine to have more people take it, if you’re concerned about safety.”
This personal risk assessment theory points to the ways Black communities are no different from white communities in terms of COVID-19 vigilance, regardless of historical instances of medical racism. “We remember the past, and if you went to a historically Black college or university, you might be more familiar with that, but we don’t live [in the past],” said Perry. “It’s historical for us: It makes us vigilant, but it doesn’t make us stupid.”
Conversely, Perry said, Black communities are disproportionately riddled with poverty. Perry shared the anecdote of a young dad he knows who earnestly cautioned Perry to “wait and see how [the vaccine] is going to work out.” Perry had been engaging with the dad through the Fatherhood Initiative at New Opportunities, a community action agency in Waterbury that offers social services to eliminate poverty and help those in need. While Perry was touched by the young dad’s concern, Perry also recognized the danger of his mindset. “I said to him, ‘If I wait to see how it’s going to work out, I might not be around to hear the outcome,’” Perry said. “We don’t have the privilege of saying we can just wait this out because it’s affecting us in such a radical way, more so than our counterparts.”
To reach younger people, the cultural ambassadors started the Young Ambassadors program, a cohort of 19- to 30-year-olds specifically affiliated with the AME Zion Church. Perry said that once the inaugural young ambassadors complete their 30 hours of YCCI training, their role will include spreading messaging on social media. “Hopefully, then we can reach another population that might be more readily interested in clinical research, including the areas of vaccines and how they may help prolong life,” he said.
While Dixwell Avenue Congregational is not directly plugged into the YCCI support network, Streets noticed similar age-related trends in his congregation. Among his members that were vaccine-eligible at that time — health care professionals, long-term care facility affiliates, and individuals 75 years and older — Streets observed generally “open and positive” attitudes toward the vaccine.
Consequently, rather than hesitancy towards the vaccine, Streets believed the larger issue facing the vaccine-eligible members of his congregation were barriers to vaccination, mainly due to barriers to technology. Thus, a paradox emerges: 20- to 50-year-olds who are more well-versed with technology tend to be more skeptical of the vaccine, while seniors who are more willing to take the vaccine tend to be obstructed by that same technology.
ENVIRONMENTAL BARRIERS TO VACCINATION
Streets identified the top three barriers to vaccination as the digital divide, the skills and informational divide and direct access — the lack of access to technology, technological literacy and secure transportation to vaccination clinics, respectively.
Streets shared the anecdote of one 90-year-old congregant who was lucky to have assistance through both her granddaughter and her home care facility, to which the vaccine was directly delivered. However, most do not have that luxury, said Streets. He estimated that at least half of the church’s elderly members do not have a close family member or friend to readily assist them, which is increasingly problematic during a time where nearly all of our daily tasks have shifted to online interfaces. Additionally, many of these members live off a fixed income, which would make upgrading to the latest technologies a superfluous expense.
Perry shared these concerns. “What are we going to do with elderly people when hospitals are closed, and the COVID is so bad that even their relatives can’t even get in to see them? And they’re having difficulty reaching their doctors?” he recalled pondering in early October. With Johnson’s support, Perry piloted a five-week program at his church where 12 seniors were given relatively cheap tablets and taught the basics of Facebook, email, telemedicine appointments, Zoom and MyChart, an application used to schedule vaccine appointments online.
“Health care institutions and academic institutions [put] the onus on the community to trust them.”
—Jessica Cerdeña
However, technology is only half of the battle. For Streets, a big shortcoming on the part of the public health and medical sector is the reluctance to extend medical therapies to BIPOC patients in environments where they feel most comfortable — namely, places of worship. “The church has always been a social service charitable institution, but the focus is now public health,” Streets said.
For those wary of getting vaccinated, places of worship are safe, hospitable spaces with built-in networks for providing transportation options, Streets said. Some churches, clustered closer to Hartford, have already begun hosting pop-up vaccine clinics. However, Streets insisted that “more collaboration is necessary — public health needs to recognize the influential role churches can play.”
An optimal example of community engagement, described by Cerdeña, is an initiative first implemented in New York in 2004 called Project VIVA where researchers went directly into neighborhoods and knocked on doors to address concerns about the flu vaccine. “When they actually worked with community-based organizations, and actually went to where people were living, working, playing, socializing, etc. to try to bring vaccines to them there, and actually listened to people’s concerns regarding the vaccine,” Cerdeña said, “that was much more effective than any kind of flyering or messaging through other avenues.”

(Regina Sung)
Cultural ambassadors have tried flyering in the past. During the fall of 2020, Perry, along with other Branford town leaders, disseminated flu vaccine information via flyers at the local food pantry. Though community-centered in some regards, flyering introduces the barrier of language. According to Cerdeña, pamphlets are rarely written at or below a seventh grade reading level, or with language reflective of the diversity of the environment. Speaking of enrollment paperwork for clinical trials, Ogbuagu echoed this frustration. “So many times the first wave of literature is always in English and then you have to scramble to get, at best, Spanish,” said Ogbuagu. “But then when you start to deal with other minority languages, it’s almost impossible.” Cerdeña noted that New Haveners are fluent in Spanish, Haitian Creole, Portuguese, Polish, Hindi, Gujarati, Farsi, Pashto and Arabic — to name a few. During a global pandemic that is affecting minority communities at disproportionate rates, efforts aimed at building trust must remain cognizant of these less conspicuous barriers.
CULTIVATING EFFORTS AND SOLUTIONS
For the AME Zion cultural ambassadors, mitigating barriers means implementing initiatives in the spaces members of the Greater New Haven African American community already engage. They organized a bi-weekly Monday segment, “The Community Health Series” on the Tom Ficklin Radio Show, which airs on New Haven broadcast station WNHH 103.5 FM. Perry is featured on most episodes, and whether he is discussing prostate cancer, cardiovascular health or COVID-19, he aims to bring information about healthier living straight to a prominent Black radio show. Similarly, the cultural ambassadors published a YCCI Ambassadors Newspaper that featured Black professionals speaking on COVID-19.
Ogbuagu credited the strength of the Cultural Ambassadors program to the credibility and influence of its community leaders. “The cultural ambassadors are the key people who play a role at the tip of the pyramid, and the base of that [pyramid] could be unlimited,” said Ogbuagu. “It’s the people who come to their churches and the people they interact with in the barbershops.”
He continued, “Because these programs are primarily within New Haven, obviously the number of people that are directly involved in the Cultural Ambassadors program is limited and finite, but the sphere of influence could be much greater.”
Ogbuagu called these efforts a “great model,” and testified to how the Cultural Ambassadors program contributed to YCCI’s greater than average minority participation in clinical trials when compared to peer research institutions.
However, the robust and creative strategies demanded to connect with the Black community may indicate that the failure of public health to sufficiently support BIPOC communities is due to a larger issue: structural racism. “When we think about why we’re seeing disproportionate rates of COVID among Black and brown populations,” Cerdeña said, “it’s because of inequities in the food system that contribute to higher rates of diabetes and hypertension, comorbidities that affect worse outcomes for people who contract COVID; it is due to inequities in housing conditions; it is due to the fact that Black and brown populations are more likely to be essential workers; it is due to the fact that for cost-saving reasons, people might be living in multi-generational households.”
When the cultural ambassadors go to work, they tackle all of these issues and more. The work is endless, said Johnson. While commendable, the constant demands on individuals to re-imagine systemic problems betrays yet another systemic problem: what Cerdeña calls the phenomenon of “health care institutions and academic institutions putting the onus on the community to trust them.” Perry personally came up with and pushed for the radio show segment; he had the foresight to anticipate technological barriers for seniors at his church. These initiatives are born from the community. The unique aspect of Perry’s ingenuity is that he has institutional support.
When health care institutions have hosted programs and events during the pandemic, they are usually aimed at fostering trust by providing information. On Jan. 26, in a virtual town hall co-hosted by the Greater New Haven NAACP and YNHH, Churchwell moderated a Zoom webinar alongside Greater New Haven NAACP President Doris Dumas. The event, titled “COVID-19 Vaccine: The Facts vs. Fiction,” was attended by about 200 YNHH patients and New Haven residents. With a panel of emergency doctors, YCCI representatives and the Rev. Perry on behalf of the cultural ambassadors, the goal was to address vaccine hesitancy from all sides.
(Regina Sung)
This collaborative effort by an array of health care professionals to directly appeal to communities is one positive that has emerged from the pandemic. “Forget clinical research, there’s this larger problem: this mistrust of even the medical community in general — health care systems, hospital systems, medical research as a blanket issue,” Ogbuagu said. “I like that COVID-19 has unmasked this. Even in the routine course of the services that we provide to our communities, we need to engage our community. We need to involve them more in what we do.”
Still, holding an event over Zoom does not solve the problem of access, given the prerequisites of attendees having Wi-Fi, a technological device, technological literacy, English comprehension and being plugged into certain networks to hear about the event in the first place. Come-one come-all Zoom events also don’t relieve community leaders of the responsibility to provide truly accessible options — though this is not a concern for Perry.
“The more I branch out, the more people will see. It’s not limited to AME Zion. It’s just that we’re starting here to branch out,” Perry said. “You can never start with the general because it has no foundation, and I think the foundation that we’re starting with is a foundation that has historical legitimacy.”
THE PROBLEM WITH ‘HESITANCY’
Nevertheless, when asked how they were receiving their information about the vaccine, the first response from the Dixwell congregants came via Zoom chat: “Facebook!” The sender was half-joking, but still, responses varied between “television” and “word of mouth.” The only Dixwell member who testified about a vaccine-learning experience facilitated by public health professionals was a young person who attended a Sickle Cell Disease Association of America of Southern Connecticut town hall. She attended because of her underlying condition — and the fact that she had reacted poorly to one-size-fits-all therapies in the past.
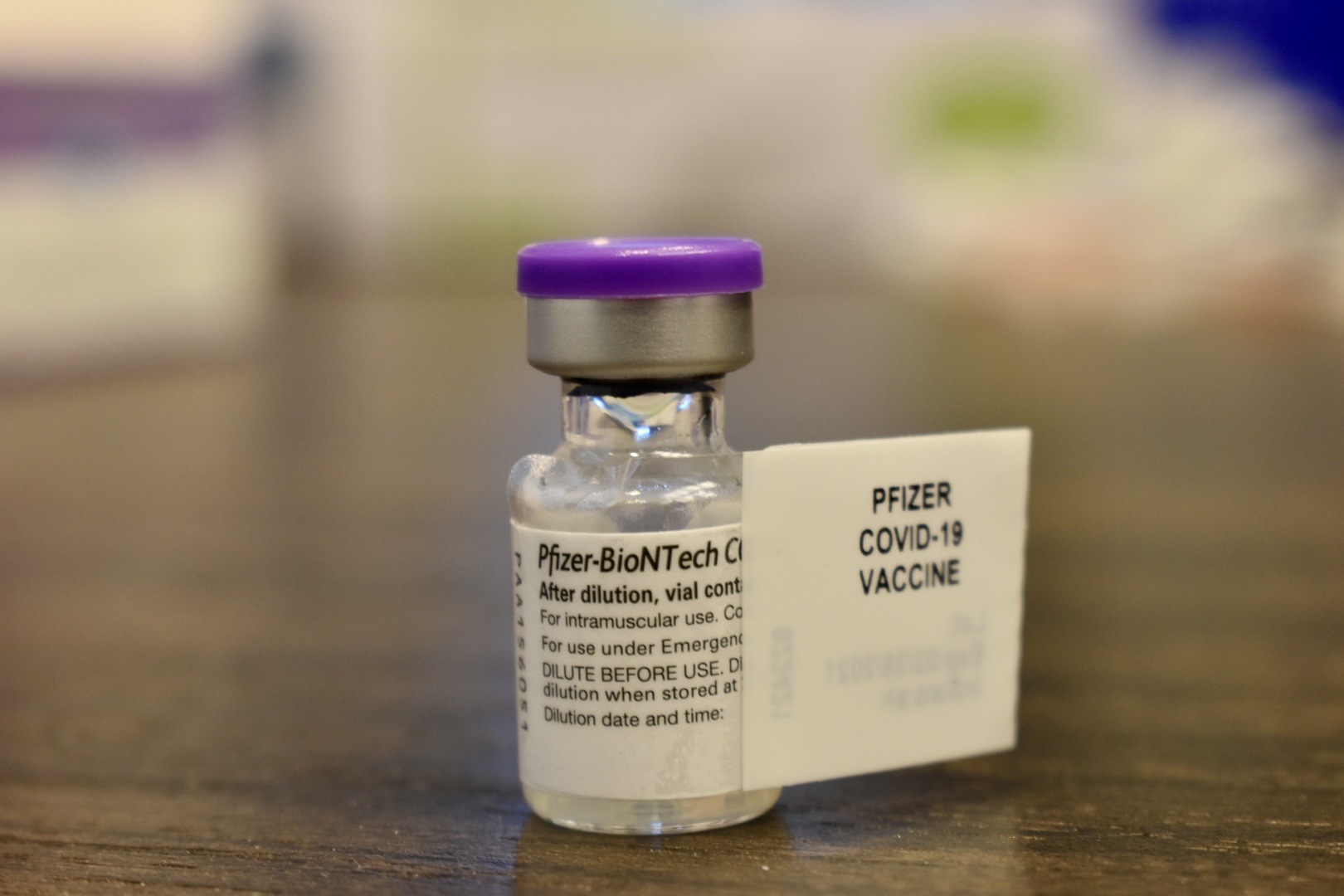
Likewise, it seemed that the only congregants who would pass on the vaccine once offered were those with preexisting conditions. Generally speaking, these congregants had previously undergone bad medical experiences related to their preexisting conditions; they seemed the most well-informed about the potential adverse effects of the vaccine. For example, one woman said she opted for the Pfizer vaccine over the Moderna vaccine because Pfizer had lower rates of adverse side effects during clinical trials. After one man expressed concern about reputable sourcing of information, this same woman informed the group about the daily COVID-19 updates residents can receive via phone call from their local health departments.
In contrast to others’ skepticism, one elderly member proclaimed, “The shot or death!” While members of the group laughed, the sentiment struck a salient chord. For many, said Churchwell, COVID-19 is extraordinary in that the adverse effects of not taking the shot are much greater than, say, not getting your annual flu shot. Any outsized focus on minority vaccine hesitancy undermines this intuitive fact.
Most Dixwell members said they called their primary care doctors straight away once they were vaccine-eligible and only turned to “word of mouth” when the primary care pathway wasn’t available to them. This demonstrates that the central problem surrounding vaccine hesitancy is not historical mistrust borne from repeated instances of medical racism, nor present-day health care malpractices. The central problem is racism, cemented in the Americas when white Europeans put captured Africans on ships. Vaccine “hesitancy” is a reflection of medical inequity, itself just one symptom of structural racism. So, in order to combat vaccine inequity, we must understand Cerdeña’s central dictum: “Racism is not the shark. It’s the water.”
Credits
Powered by 